IMPLEMENTATION OF THE NATIONAL TUBERCULOSIS PROGRAMME IN 2013
Analysis of the Implementation of the National Tuberculosis Programme (2012-2016) for 2013
National Tuberculosis Programme for 2012-2016 years (hereinafter – NTP) was adopted according to the Law of Ukraine dated 16.10.2012 No. 5451-IV. It is the third NTP, this one already includes other sources of funding, namely funding under the round 9 grant of the Global Fund to Fight Tuberculosis (hereinafter – GF). However, its budget does not take into account absolutely all sources of funding, including donors, such as USAID (Chemonics, MSH, SIAPS), as well as activities that are carried out within the framework of WHO and others.
Unfortunately, according to the Decree of the Cabinet of Ministers of Ukraine dated 31.01.2007 No. 106 "On Approval of the Procedure of the Development and Implementation of State Targeted Programs” the standard structure, form and approaches to compiling of all state targeted programs were approved that limit the possibility of taking into account the individuality of various Programs. In this connection, there are restrictions on changing the structure and form of the Programs. The Ministry of Economy does not coordinate the Programs with a budget deficit. The above regulatory constraints make it impossible to include to the NTP all activities and the budget required to combat TB, i.e. to show the budget deficit, which would allow seeing the complete picture of the financing, including the problem areas in order to attract more attention to the problem of TB within the country, as well as international donors.
Ukraine has never conducted a detailed calculation of the necessary budget for all TB activities, which would have shown the required budget for TB combating, which would allow seeing the budget deficit, inefficient use of resources and others. To calculate the budget for all TB activities the World Health Organization developed the corresponding tool.
There also are no flexible mechanisms to revise the NTP. In 2013, Rinat Akhmetov Foundation for Development of Ukraine initiated the process of revising the NTP. The Program has been revised to include the necessary and important activities for a full-fledged fight against TB. Unfortunately, the improved NTP has not yet been approved.
Over the entire period of its activity, NTP for 2012-2016 presupposes financing from the state budget 1,236,478.4 ths. UAH (incl. by year – see tabl.1).
Table 1. Planned and allocated financing for the NTP from the state budget for 2012-2016 years.
|
Year |
Planned by TB Program |
Allocated according to TB Program |
|
2012 |
199,546.43 ths. UAH |
199,546.43 ths UAH |
|
2013 |
241,305.87 ths. UAH |
216,599.27 ths UAH |
|
2014 |
254,037.27 ths. UAH |
|
|
2015 |
263,311.64 ths. UAH |
|
|
2016 |
278,277.19 ths. UAH |
|
The state budget provides a centralized procurement of anti-TB drugs, consumables for microbiological diagnostics of tuberculosis and X-ray equipment.
The graph below shows the dynamics of planned and allocated funding from the state budget according to the TB Program for the period from 2009 to 2016 (Figure 1).
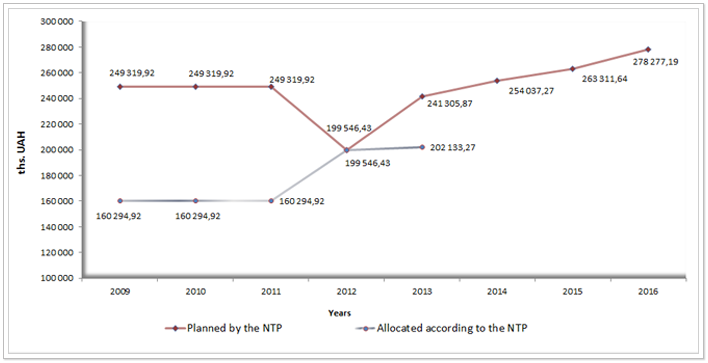 Figure 1. Planned and allocated funding for the TB Program in Ukraine from 2009 to 2016. (ths. UAH)
Figure 1. Planned and allocated funding for the TB Program in Ukraine from 2009 to 2016. (ths. UAH)
As can be seen from the graph only in 2012 the planned sum from the state budget for TB combating was allocated. Under the approved NTP for 2013 the volume of the annual budget – 353,881.43 ths. UAH – was approved actual funding is 467,045.20 ths. UAH* (State Service report, Appendix 3), i.e. it was allocated 32% more than it was planned in the NTP. Overfulfillment of the funding occurred at the expense of the local budget, as “digital” funding was not provided for in the budget of the Program, i.e. the volume of the funding from the local budgets is determined separately within the expenditures of the local budgets, as well as from other budgets and donor funds.
The actual funding of the NTP in 2013 was made in the amount of 467,045.20 ths. UAH*, where 43.0% - from the central budget, 54% - from the local budgets and 3% from other sources. Underfunding of the NTP in 2013 was due to the lack of financing from the state budget by 16% (241,305.87 ths. UAH were planned, but actually 202,133.44 ths. UAH were financed), as well as due to underfunding from other sources by 87% (112,575.56 ths. UAH were planned, and actually 15,025.97 ths. UAH were funded). However, the total amount of the budget spent in 2013 for TB combating according to the NTP was significantly higher, as the report on the TB Program did not include the data on financing under the Global Fund grant, which was planned for 2013 in the amount of 112,575.56 ths. UAH, but was used in the amount of 87.261.28 ths. UAH in 2013, the economy was re-budgeted for the additional purchase of second-line anti-TB drugs, which is associated with an increase of cases of multidrug-resistant tuberculosis (MDR-TB). Having summed all sources of funding for TB activities (the NTP did not include USAID project budgets), we see that 554,306.48 ths. UAH was allocated for the fight against TB in 2013. Also, if we take into account the Global Fund resources, which were used in 2013 (87,261.28 ths. UAH), the budget allocation according to the TB Program is as follows (see. Pie chart in Figure 2).
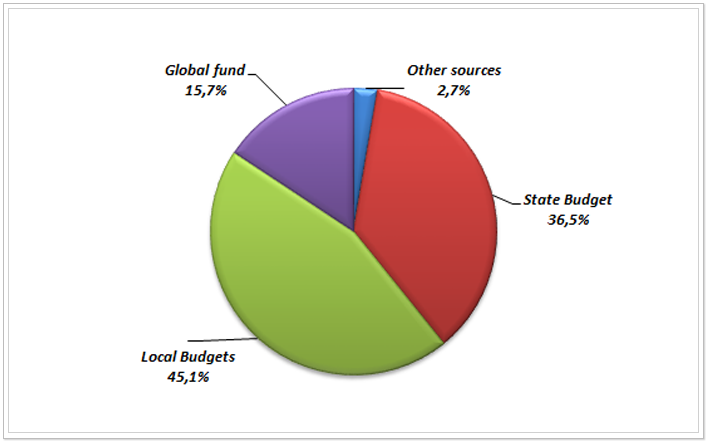 Figure 2 Percentage ratios of the different sources of funding of the TB Program for 2013.
Figure 2 Percentage ratios of the different sources of funding of the TB Program for 2013.
Thus, the NTP was actually funded from the state budget by 84% (241,305.87 ths. UAH were planned, but 202,133.44 ths. UAH were financed). The following activities were under-funded from the state budget:
- Purchase of equipment and consumables for TB diagnosis by sputum smear microscopy and culture on solid culture media (5,779.14 ths. UAH were planned, but 0.0 ths. UAH were financed),
- Purchase of consumables for the diagnosis of TB patients of category 1-3 by culture on liquid culture medium by 42% (24,252.38 ths. UAH were planned, but 14,005.80 ths. UAH were financed),
- Diagnosis and monitoring of the effectiveness of treatment with the help of X-ray and other methods of examination, in particular the purchase of equipment (21,100.00 ths. UAH were planned, but 0.0 ths. UAH were financed),
- Access to the prevention and treatment of patients of category 1-3 by standard schemes, such as the purchase of the required amount of first- and second-line anti-TB drugs by 67% (53,192.31 ths. UAH were planned, but 16,711.66 ths. UAH were financed), and
- Introduction of innovative methods of rapid diagnosis of TB, including MDR-TB, in II-III level laboratories by molecular genetic methods, in particular the purchase of equipment and consumables by 100% (1,852.99 ths. UAH were planned, but 0.0 ths. UAH were financed).
It is important to emphasize that the underfunding of procurement of anti-TB drugs for category 1-3 of patients in the amount of 36,480.65 ths. UAH was justified by the need to use large remains of anti-TB drugs since the last year, received free of charge under the grant from the Global Drug Facility (combined anti-TB drugs). However, the money saved was not spent in full for the purchase of second-line anti-TB drugs for patients suffering from MDR-TB, but only 25% - 9,207.5 ths. UAH. Since only 167,881.89 ths. UAH was budgeted for second-line anti-TB drugs for patients suffering from MDR-TB in 2013, this amount was not enough considering the growth of MDR-TB cases in the country, even taking into account the fact that it was financed by 5% more than it was planned - 177,089.4 ths. UAH. This example shows, how it is important to be able to review the budget of the NTP each year and to adjust it according to the epidemiologic data and other changes, so that it meets the real needs and is used to optimum effect.
The NTP for 2012-2016 consists of 8 main tasks, each of which includes specific measures with parameters.
The first task of the NTP – improvement of the health system in the sphere of combating TB, including MDR-TB was executed by 100% (20 of 20 in accordance with the State Service report on the TB Program.
However, the model of health care reform in the sphere of combating TB has not yet been tested in pilot regions. In 2014 piloting of models is performed in several regions. In the Donetsk region piloting was made possible by the support of the Charitable Foundation “Development of Ukraine” and in Dnepropetrovsk, Vinnitsa and Poltava regions – thanks to the support of the USAID-funded “Strengthening TB Control in Ukraine” project. By the end of 2014 the results of these pilot projects will become available.
In addition, the implementation of the NTP first task for 2013 involved improvement of the regulatory basis to ensure the effective functioning of the procurement of anti-TB drugs, their rational allocation and monitoring of their use. This resulted in approval of the Order of the Ministry of Health of Ukraine dated 22.02.2013 No. 156 “On Amendments to the Procedure of Calculating the Need for anti-TB drugs”, registered with the Ministry of Justice of Ukraine on 22.03.2013 under No. 464/22996. However, it has a number of drawbacks that limit the access of patients with tuberculosis to anti-TB drugs, namely, a diminished prescription coefficient of second-line anti-TB drugs, thus, for Capreomycin it is only 15%, with the actual need for this drug about 25% (in the treatment regimens of patients under the Global Fund grant the 25% coefficient of need for Capreomycin was used since 2012). Besides the procedure includes the coefficient of “loss” of MDR-TB patients, i.e. initially drugs are calculated not for all patients suggesting that 8% of patients will refuse from treatment or die, which contradicts the international approaches to the calculation of anti-TB drugs, etc.
As mentioned above, due to the absence of a flexible mechanism for revision of the NTP, in the context of growth of MDR-TB incidences, the NTP planned budget does not meet the needs of the country, i.e. growing number of patients with multi-drug resistant TB (2011 – 4305 patients, 2012 – 6934 patients and 2013 – 9650 patients). The increase in MDR-TB case-finding occurred in 2012-2013 thanks to the training of medical personnel in new diagnosis algorithms, keeping of reporting documentation, introduction of new methods of diagnosis, mainly under the round 9 grant of the Global Fund. And this is not the limit for case-finding of multi-drug resistant forms that the WHO will confirm in its next report, giving the estimated data on the number of multi-drug resistant TB forms based on the results of the study of the prevalence of multidrug-resistant tuberculosis strains in Ukraine, which is to be finished by the end of 2014. It should be noted that by planning the NTP in 2011 no one could predict such an increase of MDR-TB incidences and plan the appropriate funding for second-line anti-TB drugs.
The above mentioned drawbacks led to disruptions in the availability of complete schemes of second-line drugs in 2013, which was repeatedly confirmed by citizens' appeals on this issue at the All-Ukrainian TB hotline, supported by Rinat Akhmetov Foundation for Development of Ukraine.
Also in 2013, another Order of the Ministry of Health of Ukraine was adopted dated 26.07.2013 No. 650 “On Approval of the Methodology for determining the financial quotas for administrative-territorial units for centralized procurement of anti-TB drugs” registered with the Ministry of Justice of Ukraine on 15.08.2013 under No. 1408/23940. The basis for this document is the distribution of financial quotas by regions of Ukraine within the approved funding under the NTP. Financial constraints on the TB Program do not allow the purchase of anti-TB drugs in accordance with the method of drugs calculation, which is based on the number of patients registered last year. For 2014, the financial quota for first- and second-line anti-TB drugs has been approved amounting to 154,283.1 ths. UAH (but the NTP planned amount is 170,732.2 ths. UAH), underfunding is 9.6%. In accordance with the above document 154,283.1 ths. UAH were distributed by regions for 2014. Below there is a chart which shows an uneven distribution of quotas between the regions and the fiscal deficit between quotas and the cost of the calculating application for anti-TB drugs (Figure 3).
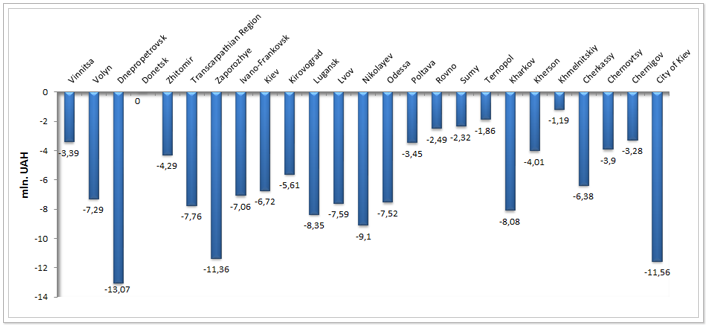 Figure 3. Budgeting deficit of the purchase of first- and second-line anti-TB drugs by the regions of Ukraine for 2014 (mln. UAH)
Figure 3. Budgeting deficit of the purchase of first- and second-line anti-TB drugs by the regions of Ukraine for 2014 (mln. UAH)
In accordance with the above order the quotas were calculated for the regions. This calculation takes into account the number of patients to be taken for treatment under the Global Fund grant.
The second task of the NTP – Improvement of monitoring and evaluation system (hereinafter - the M&E) of results of the NTP implementation, was performed by 57% (4 of 7 subtasks according to the report on the NTP).
Unfortunately, at this stage it is impossible to create fully working monitoring and evaluation departments, as the Regulation on regional M&E departments has not yet approved and the staff schedule of these departments has not yet revised.
The All-Ukrainian electronic TB case-based data manager in the penitentiary system has not yet implemented, despite the fact that under the GF grant 43 personal computers were purchased, the connection to the Internet was made and professionals underwent training (with technical support from MSH).
MDR-TB reporting forms approved by the Order of the Ministry of Health dated 07.03.2013, No. 188 do not conform to WHO recommendations regarding the principle of registration and the outcomes of MDR-TB treatment.
Monitoring visits from the national level to the regional one were carried out in 27 regions of Ukraine, but only once, despite the fact that the two-time visits were scheduled under the GF grant. Single visits are extremely insufficient at such low levels of therapy effectiveness for 2013 among new cases – 67.5% (target – 85%), among recurrent cases – 42.2% (target – 85%), among MDR-TB cases (cohort of 2011) – 34.2% (target – 75%), with low coverage with testing of patients for drug susceptibility to first-line anti-TB drugs – 47.8% and so on.
Single monitoring visits from the regional level to the regional one were made in 68.9% of cases, which is extremely low for M&E of all TB activities at the district level.
Also, there has not yet been approved any algorithm and a tool for carrying out of monitoring visits at all levels, including all approaches in the fight against TB (case-finding, diagnosis, treatment, monitoring and evaluation, infection control, management of medicines and pharmacovigilance), although the country has several variants of tools for such monitoring of TB activities.
The third task of the NTP – Organization of the activity on TB case-finding and diagnosis, was performed by 7% (1 of 14 subtasks according to the report on the NTP).
The laboratory equipment was not purchased from the state budget, only consumables were partially purchased by 58% for TB diagnosis in the liquid media. And only at the expense of consumables purchased under the GF grant, it became possible to achieve coverage of patients of category 1-3 by culture on the liquid culture medium in 72%.
In the penitentiary sector the coverage with TB diagnosis in the liquid media reached only 49% of the planned number of patients.
Tuberculin diagnostics in children from 4 to 14 years accounted for only 54%. This low percentage of coverage of tuberculin diagnostics may lead to an increase of TB incidences among children in the future.
The fourth task of the NTP - TB treatment and prevention, was performed by 67% (6 of 9 subtasks according to the report on the TB Program).
None of the regions of Ukraine received money for proper nutrition in hospitals in accordance with the Decree of the Cabinet of Ministers of Ukraine dated 27.12.2001 No. 1752 “On the principles of nutrition for persons with tuberculosis and infected with Mycobacterium tuberculosis” – 43.5 UAH per patient based on 2013 average prices. But on average, only 21.3 UAH per patient was allocated. Increase of the sum for nutrition of one patient can be achieved by reducing of bed capacity without any additional increase in the budget in accordance with the Order of the Ministry of Health dated 10.07.2013 No. 584 “On approval of the instructions for calculating the optimal bed capacity in specialized TB facilities providing inpatient care for TB patients”.
The percentage of TB patients among detainees and prisoners who did not interrupt treatment was 62% (target – 70%), despite the social support of this cohort within the implementation of the project at the expense of the Global Fund grant.
The percentage of TB patients of category 1-4 who underwent controlled outpatient treatment was - 73.3% (target - 75%). These data were presented on the basis of reports from the regions according to the TB Program, but during monitoring visits the percentage of patients covered by the controlled outpatient treatment was much lower due to the limited regional budget for the social support of TB patients. The GF grant covered with social support only 10% of patients of category 1-3 who were at risk of treatment interruption and of MDR-TB patients who received treatment under the Global Fund grant (about 12% of MDR-TB patients registered in 2013).
The fifth task of the NTP – combating TB with multidrug resistance, was performed by 56% (10 of 18 subtasks according to the report on the NTP).
From time to time in 2013 there were interruptions and significant delays in the supply of second-line anti-TB drugs, which led to violations of treatment regimens and, as a consequence, of aggravation of resistance profile of mycobacteria in a TB patient. At the regional level there were sometimes problems with the lack of ability to prescribe an adequate scheme to fit the profile of resistance of the patient, confirmed by patients’ calls at the National TB hotline (0 800 50 30 80). This problem is related to the fact that anti-TB drugs are purchased not by schemes but by individual drugs and suppliers constantly violate the terms of their supply. It is important to note that under the GF grant drugs are purchased by schemes, thus allowing the patient to have guaranteed complete treatment for the whole duration of the therapy. Therefore, there is an urgent need to change the principle of public procurement of anti-TB drugs in order to purchase drugs by schemes, to implement the mechanism of rigid fine sanction for late delivery of the drugs, thereby minimizing the risk of giving incomplete and, therefore, ineffective treatment regimens.
In all regions, departments for patients with MDR-TB are established, but not all of them meet the standards of infection control, which leads to the cross-infection of patients with TB mycobacteria and, as a consequence, it aggravates the resistance profile of TB mycobacteria of the patient, i.e. there is nosocomial infection of patients with other TB strains. To exclude cross-colonization, international experts recommend implementing an outpatient model of patient care.
The percentage of MDR-TB patients who receive the social assistance only amounted to 29.9% (target – 60%). Social support for patients was assigned to the regional and district budgets, but the goal was not achieved, due to limited funding or absence of budget allocation lobbying for this activity.
The NTP encompassed the planned purchase of equipment for 76 laboratories of levels II and III, which provided quick TB diagnosis. Under the budget of Rinat Akhmetov Foundation for Development of Ukraine and the GF grant 32 systems for the rapid TB diagnosis GeneXpert were purchased for all regions of Ukraine and 2 equipment system for linear probe assay (HAIN) in the amount of about 11 mln. UAH. The equipment screened around 30 ths. patients. From the state budget there was no funding for this activity, as well as for other laboratory equipment.
According to the report on the TB Program the percentage of patients with new cases of MDR-TB who started treatment in accordance with the approved schemes was 85.5% (target – 75%), but only 49% of patients recovered (WHO target – 75%), such a low percentage of effectively treated patient is also associated with limited access to anti-TB drugs throughout the course of treatment and insufficient coverage of patients with social support during treatment.
In 2012, a WHO expert developed the “Operational Plan to combat MDR-TB in Ukraine for 2013-2014”, which unfortunately was not approved by the Order of the Ministry of Health, losing its relevance in 2013. Below there is Table 2 from the above mentioned plan, with the calculations to cover the financing of purchases of second-line anti-TB drugs from different sources as of 2012.
Table 2. Estimated number of MDR-TB patients without access to treatment due to the lack of second-line drugs, 2012-2015.
|
Names of indicators |
Planned (targets) |
|||
|
|
2012 |
2013 |
2014 |
2015 |
|
1. Number of MDR-TB * patients confirmed in the specified year (target: 100% involvement in treatment) |
5690 |
5940 |
6190 |
6440 |
|
2. Expected number of cases of patients undergoing the full course of treatment (by a source of funding): |
||||
|
a. Provision with drugs under the Global Fund grant ((3))) |
720 |
960 |
2000 |
2480 |
|
b. MSF (Doctors Without Borders) (only prisoners in Donetsk) ** |
200 |
300 |
300 |
300 |
|
c. Ministry of Health *** |
2200 |
2200 |
2200 |
2200 |
|
In total |
3120 |
3460 |
4500 |
4980 |
|
3. Number of MDR-TB patients without access to the full course of treatment (gap between the need (first line) and expected cases of the full course of treatment that will be available (second line fully)) |
2570 |
2480 |
1690 |
1460 |
|
4. Number of MDR-TB patients without access to the full course of treatment as a percentage ratio of confirmed MDR-TB patients ((point 3/point 1)* 100%) |
45% |
42% |
27% |
23% |
* Including civil and prison sectors.
** Personal communication on April 27, 2012, Dr. Yuliya Chistyakova, MedCo Ukraine representative, MSF OCB – Ukraine.
*** If the current investment is maintained. Please note that manufacturers supplying drugs to the MOH are not obliged to follow WHO quality standards and the Ministry of Health buys second-line drugs only for the civil sector.
The operational plan to combat MDR-TB in Ukraine had to be revised taking into account the changed situation with MDR-TB in the country, to approve by the order of the Ministry of Health, to use when making changes to the NTP and filing a grant application to the Global Fund as for TB/HIV component in 2014. If we make the appropriate changes to Table 2 that are relevant at the moment, we will see the real picture of the deficit of second-line anti-TB drugs in Ukraine, leaving the level of MDR-TB case-finding at the 2013 level, despite the fact that the further increase in MDR-TB cases is predicted (Table 3).
Table 3. The actual (2012-2013) and estimated (2014-2015) number of MDR-TB patients without access to treatment due to lack of second-line drugs, 2012-2015.
|
Names of indicators |
Planned (targets) |
|||
|
|
2012 |
2013 |
2014 |
2015 |
|
1. Estimated number of MDR-TB cases, according to WHO data (target: 100% involvement in treatment) |
6700 |
6700 |
6700 |
6700 |
|
2. Number of MDR-TB reported cases |
6934 |
9650 |
9650 |
9650 |
|
3. Expected number of cases of patients undergoing the full course of treatment (by a source of funding) |
||||
|
a. Provision of drugs by the Global Fund grant ((3))) |
780 |
960 |
3136 |
5250 |
|
b. MSF (Doctors Without Borders) (only prisoners in Donetsk) * |
200 |
300 |
300 |
300 |
|
c. Ministry of Health ** |
2200 |
2200 |
2200 |
2200 |
|
In total |
3180 |
3460 |
5636 |
7500 |
|
4. Number of MDR-TB patients without access to the full course of treatment. It is a gap between the need – number of reported cases (second line) and expected cases of the full course of treatment that will be available (third line fully)) |
3754 |
6190 |
4014 |
2150 |
|
5. Number of MDR-TB patients without access to the full course of treatment as a percentage ratio of confirmed MDR-TB patients ((point 4/point 2)* 100%) |
54% |
64% |
42% |
22% |
* Personal communication on April 27, 2012, Dr. Yuliya Chistyakova, MedCo Ukraine representative, MSF OCB - Ukraine
** If the current investment is maintained. Please note that manufacturers supplying drugs to the MOH are not obliged to follow WHO quality standards and the Ministry of Health buys second-line drugs only for the civil sector.
Table 3 shows that about 42% of patients with MDR-TB will not undergo the proper treatment with second-line anti-TB drugs in 2014, and about 22% of patients with MDR-TB – in 2015.
The NTP in 2014 included an increase in funding for the purchase of second-line anti-TB drugs by 3.6% compared to 2013 and in 2015 - 5.6% respectively.
If to consider two facts that even more patients will be detected in 2014 than in 2013 and the rise in prices for medicines in 2014, not 42% (4014 patients) but much more patients will be without drugs, in spite of the increased funding of the NTP - 3.6 % and an increased purchases of second-line anti-TB drugs under the GF grant (from 2000 to 3136 treatment regimens).
In 2013, the country almost managed to achieve the target value by the percentage of primary preventive and curative health care facilities, which met the requirements of infection control - 59.2% (target - 60%). However, these data were obtained from the regional reports, but not on the basis of the results of monitoring visits at the national level in the regions of Ukraine.
The incidence rate among health care workers was 5.7 cases per 10 ths. of health care workers (target - 5.0). The purpose in the NTP is not correctly specified because health care workers cannot be ill less than the total population of Ukraine as they also are part of it and subject to the same risks in the daily life. Incidence rate in Ukraine in 2013 was 67.9 per 100 ths. of population, which is slightly higher than the incidence rate among health care workers, if the parameter is reduced to the corresponding values – 57.0 per 100 ths. of health care workers. However, it should be noted that TB incidence among health care workers of TB facilities in 2013 amounted to 848.0 per 100 ths. of health care workers that was 12.5 times greater than the incidence rate in the general population. Such a high incidence rate of TB facilities staff demonstrates the ineffectiveness of infection control measures, as only 36.7% of TB facilities comply with infection control requirements on the regional TB Program reports.
In the penitentiary sector it was planned to establish 2 units for the treatment of multidrug-resistant TB in 2013 in accordance with the requirements for infection control, but unfortunately the departments were not established.
The sixth task of the NTP - Implementation of measures to control the disease by co-infection (TB/HIV), was performed by 50% (3 of 6 subtasks according to the report on the NTP).
The Regions of Ukraine in the reports of the NTP implementation in 2013 pointed that the plan of joint measures to control the disease by co-infection (TB/HIV) was realized. However, the below listed activities which are included in this plan have not been implemented, namely:
- percentage of patients who underwent prophylactic treatment with Co-trimoxazole in 2013 in accordance with the need was 74% (target of Ukraine for 2013 - 80%, target of WHO - 100%);
- percentage of patients who were covered with antiretroviral therapy - 72.4% (target of Ukraine for 2013 - 80%, target of WHO - 100%);and
- percentage of patients suffering from TB, which were covered with HIV testing almost reached the target - 94.6% (target of Ukraine for 2013 - 95%, target of WHO - 100%).
The seventh task of the NTP - Creating a favourable social environment for the activity of civil society institutions aimed at overcoming the TB epidemic, was performed by 33% (1 of 3 subtasks according to the report of the NTP).
All regions reported on the development and approval of a regional action plan to inform and involve the public to counter TB (ACSM strategies), but in accordance with the decision of the Regional Council on combating TB, HIV infection and AIDS dated 11.12.2012 in Zhytomir Region ACSM strategy was not approved but directed for follow-up revision. By the end of 2013 ACSM strategy was not adopted in this region.
The target was not achieved as for the number of regions (2013 - 17/18 regions) which organized and conducted training for employees of local governments, social workers, volunteers, medical nurses and health visitors, businessmen on counselling of population to change behaviour and the formation of a conscious attitude to TB prevention and treatment.
The eighth task of the NTP – Study in the framework of the NTP to evaluate the effectiveness of the NTP activities through the peer review, was not performed, but postponed to 2014.
Also for 2014 it was planned to conduct a comprehensive external evaluation of the national activities to combat TB in Ukraine by WHO experts. The assessment will be carried out with the technical support of Rinat Akhmetov Foundation for Development of Ukraine.
Summary
The NTP for 2012-2016 includes 8 large-scale problems. For 2013 78 activities were planned, only 45 were carried out, which was the implementation of the NTP by 58%. Performance of NTP tasks is shown in Figure 4. It should be noted that the analysis of most of the activities was based on the reports from the regions on their implementation of the NTP that involved some subjectivity. The NTP was actually financed from the state budget by 84%. To assess the adequacy of financing of TB activities in Ukraine, taking into account all sources of funding is not possible, because the detailed calculation of the necessary funding has been never performed.
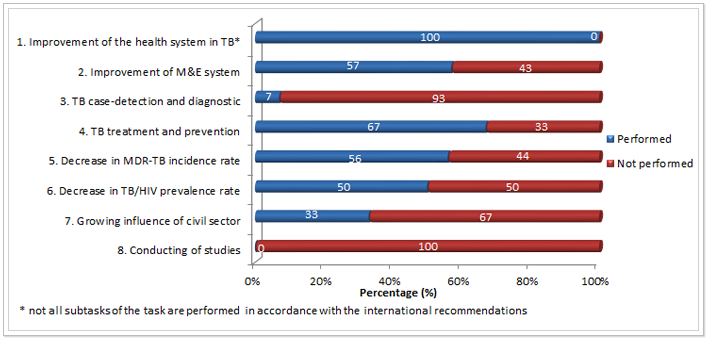 Figure 4. Performance of the TB Program tasks in 2013 (%)
Figure 4. Performance of the TB Program tasks in 2013 (%)
Among the main reasons for underperformance of the goals set are the following: lack of funding from the state and local budgets, inertia of the legal framework (transition to international approaches to TB and MDR-TB management is very slow), lack of a research base, which results should be the main lever of lobbying of making changes during TB service reforms in Ukraine, taking into account economic efficiency.



